Follow The Truth, Not The Fake News
We All Want to Follow the Most Accurate Science in Our Struggle Against Infectious Disease, to that end Please Consider Reviewing the Following Articles from Various Outlets.
MASK TOXICITY – German study exposes dangers of CO2 re-breathing – neuron death & learning impairment (children), stillbirths & birth defects (pregnant women), testicular toxicity (adolescents)

On March 3, 2023, a German team published an extensive review of MASKING during the COVID-19 pandemic that should put the final nail in the coffin of masking & mask mandates.
The Kisielinski Study
A German team, led by an Independent Surgeon in private practice, published a large review of MASK use during COVID-19 pandemic.
It has 172 references.
I will summarize key findings:
- 4.5 billion people (58%) were confronted with a “mask obligation”
- Fresh air has 0.04% CO2
- Wearing masks more than 5 minutes: 1.4 to 3.2% CO2
Carbon Dioxide Re-breathing
- Surgical mask after 30 min = 2.8-3.2% CO2 (U.Butz, 2005)
- N95 after 1 min = 0.9% CO2 (T.Blad, 2020)
Why isn’t the CDC warning parents that masking their kids creates unacceptably high levels of CO2?
Del Bigtree was right. The CO2 levels in masks worn by kids rises to over 13,000 ppm. This is above the normal 1,000 ppm level, and significantly above the 2,000 acceptable level. The CDC is silent.


UK – Cochrane Study Proves Masks do not work
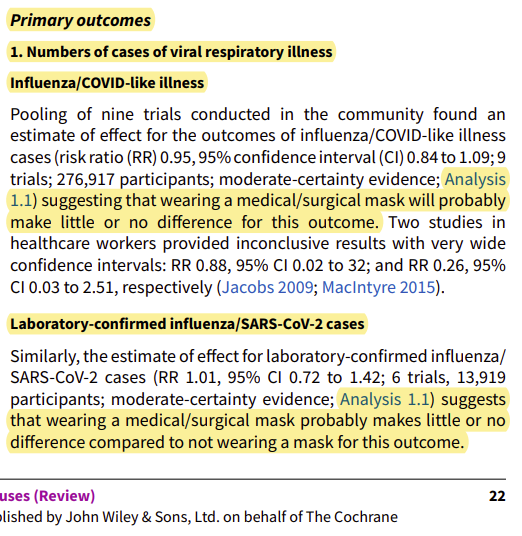
Thanks to Stephen Petty for bringing the new Cochrane Review entitled, “Physical interventions to interrupt or reduce the spread of respiratory viruses (Review)” to my attention this morning.
He wrote: “Once again, masks and N95s don’t work – see marked pages 22-23”
From page 22:
 |
From Page 23:
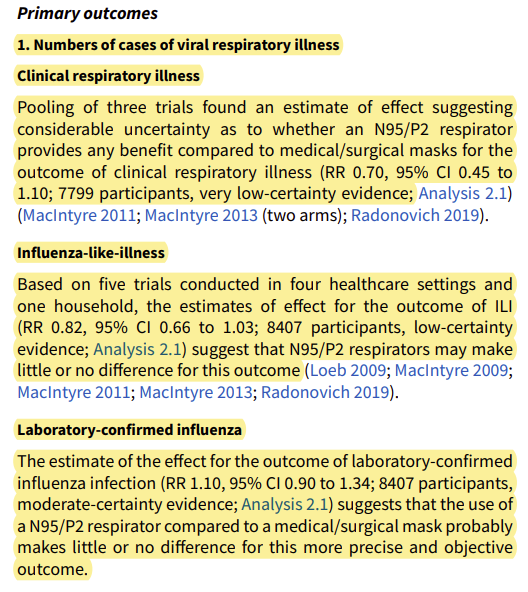 |
The Cochrane press release confirmed all this and then concluded: “We are uncertain whether wearing masks or N95/P2 respirators helps to slow the spread of respiratory viruses.” Yeah right. Let me provide the Plain English Translation for you of that statement:
“We couldn’t find a shred of evidence supporting the notion that masks make any difference whatsoever. Whoever is advising people to do this is not basing their decision on any scientific evidence.”
The Bangladesh mask study
I personally was most impressed with the Bangladesh mask study which claimed masks work. Here is the curve for the purple cloth masks vs. placebo. If you can see a difference between the two, you should immediately apply for a job with the CDC:
 |
Additional MASK Information as Provided Below
Mask-wearing is unhealthy and has the potential for great harm and loss of life
First of all, masks don’t stop viruses. Any virus. It even says so on the box of blue masks you pick up at Target.
Secondly, they’re harming people. They increase CO2 levels and decrease oxygen intake. A comment on this website stated:
I am President of a Manufacturing Company in Saskatchewan, Canada. Under Saskatchewan Occupational Health & Safety Rules it is illegal for me to expose any of my Employees to a Hazardous Environment, above 1,500 ppm CO2 levels (Atmospheric is 375 to 400 ppm), or below 19.5% Oxygen levels (Atmospheric Oxygen is 20.9%). OSHA Safety Officers have measured Oxygen levels at 17.4% behind an N95 mask with an IBRID 6 Gas Monitor. Del Bigtree, Medical Research Journalist measured CO2 levels between 8,000 to 10,000 ppm behind a cloth mask and over 10,000 ppm behind an N95 mask which is Hazardous Environment!
If masks do, indeed, restrict oxygen and increase CO2, there may be other unintended consequences. Miscarriages and stillbirths rose over 300% during a six-week period in early 2021. Obstetricians also report smaller umbilical cords, which indicates that the pre-born baby isn’t getting all the oxygen (via the placenta) that he/she should have.
Both emotional and physical health is being harmed by the use of masks. Clearly, these are not in the interest of life.
Read the entire article at LifeSiteNews.com
Rense.com published this study of mask wearing Hypoxia, and Hypercapnia
Masks, False safety and real dangers, Part 3:
Hypoxia, hypercapnia and physiological effects
Boris Borovoy, Colleen Huber, Maria Crisler
Abstract
Wearing a mask causes physiological changes to multiple organ systems, including the brain, the heart, the lungs, the kidneys and the immune system. We examine changes in oxygen and carbon dioxide concentrations in masked airspace that is available to the airways over the first 45 seconds of wear. Our findings of reduced oxygen and increased carbon dioxide in a masked airspace are not inconsistent with previously reported data. We also consider the range of injuries known to occur to the above-named organ systems in a state of hypoxia and hypercapnia. As an excretory pathway, carbon dioxide release by cells throughout the body, and then past the alveoli and then the airways and orifices, has not been previously challenged by deliberate obstruction in the history of the animal kingdom, except for relatively rare human experiments. Self-deprivation of oxygen is also unknown in the animal kingdom, and rarely attempted by humans. We examine the physiological consequences of this experiment.
MASKS and HYPERCAPNIA Do masks cause systemic hypercapnia? Airway obstruction is a long recognized cause of retention of carbon dioxide and respiratory acidosis. A sustained level of increased carbon dioxide stays inside of masked air, compared to room air, which in turn sustains a low level of hypercapnia. Rebreathing of exhaled air has been found to quickly elevate [CO2] in available air above 5000 ppm, and to increase arterial CO2 concentration and to increase acidosis.1 The mechanism of mask-induced hypercapnia may also include the moisture on a mask trapping carbon dioxide from exhalation. Some carbon dioxide diffuses in the air, more so if dry, but some portion of it, trapped by water vapor and mask moisture, would form a weak, unstable acid with water, for re-circulation to the airways and lungs. The mechanism is that retention of CO2 causes an increase in PCO2. This is the primary disturbance in respiratory acidosis. It results in an increased concentration of both HCO3- and H+, which is measured as a lower pH.
Masks increase respiratory drive and bronchodilation in mild hypercapnia, from sensitive chemoreceptors picking up changes in pH of cerebrospinal fluid. Ultimately in severe hypercapnia, respiratory drive is actually depressed.
Hypercapnia is widely recognized to be an independent risk factor for death. 2 3 4 5 A number of organ systems are negatively impacted, including the brain, heart, lungs, immune system and musculoskeletal system. 6 7 2
How quickly do masks increase carbon dioxide in the masked airspace?
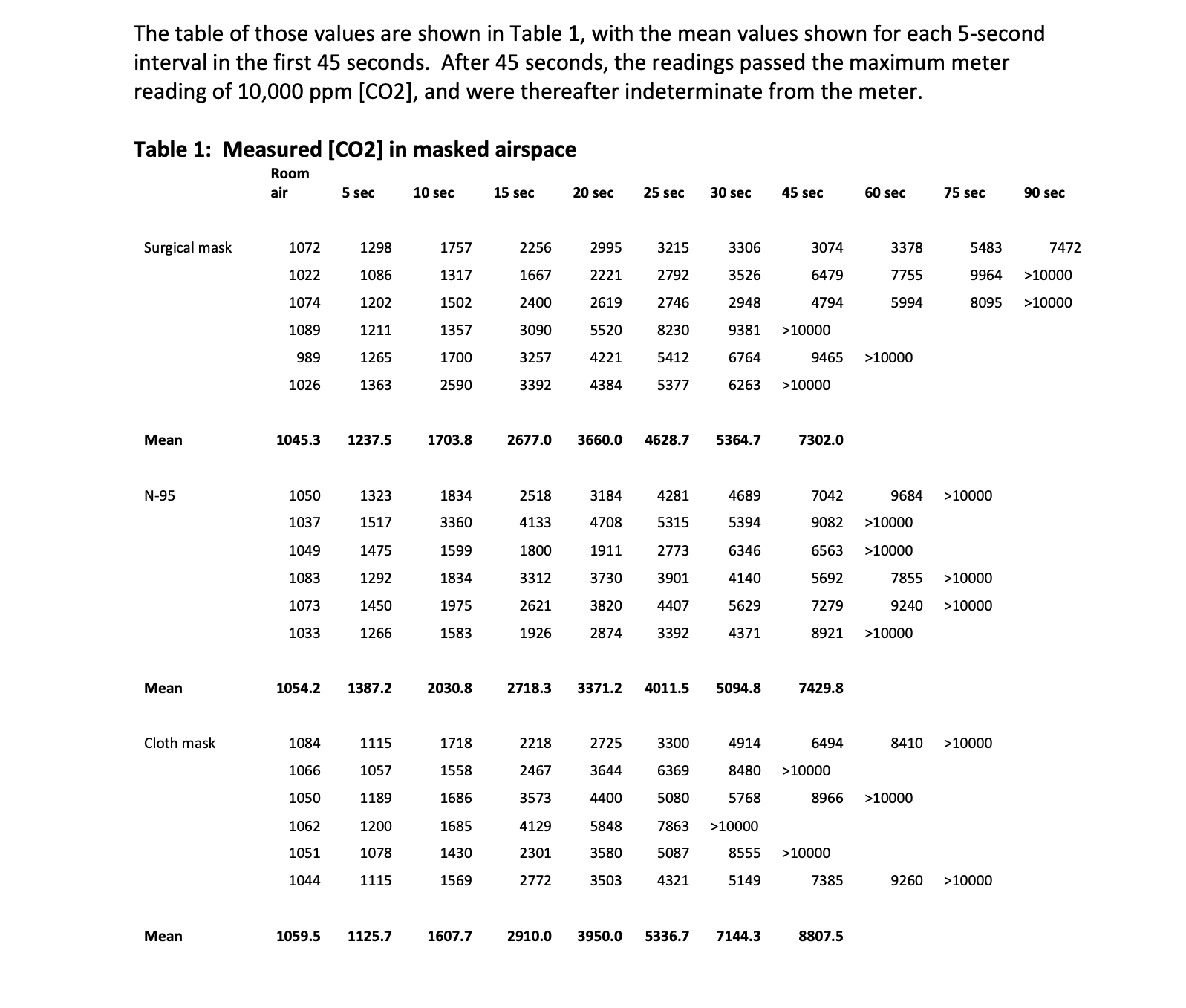
We used a new calibrated carbon dioxide meter to measure ambient carbon dioxide in room air, and then inside the masked airspace of three different masks after donning each in turn. This experiment involved a disposable surgical mask, a N-95 mask and a cloth mask.
We recorded carbon dioxide parts per million inside the masked airspace. The meter refreshed its readings at 5-second intervals, and we used those same intervals in recording CO2 parts per million. The maximum CO2 reading on the meter is 10,000 parts per million. The table of those values are shown in Table 1, with the mean values shown for each 5-second interval in the first 45 seconds. After 45 seconds, the readings passed the maximum meter reading of 10,000 ppm [CO2], and were thereafter indeterminate from the meter.
Table 1: Measured [CO2] in masked airspace Room air
If we look at the time in which our readings did not yet exceed the maximum of the meter, then we have the following graph, Graph 1, of the average rise in carbon dioxide concentration inside the masked air for each mask, as [CO2] rose over the first 45 seconds of wear.
